
Introduction
A cerebrovascular accident (CVA) is an acute disruption of cerebral blood flow. Approximately 85% of cases are ischemic (caused by blockages), and 15% are hemorrhagic (resulting from blood vessel ruptures). Early recognition and timely treatment are critical to minimizing morbidity and mortality. 1, 2, 3
Types of stroke
-
Ischemic Stroke: The most common type, caused by blood clots obstructing blood vessels, preventing oxygen and nutrients from reaching the brain. Subtypes include:
Hemorrhagic Stroke: Caused by the rupture of blood vessels, leading to bleeding within the brain. Common causes include aneurysms and arteriovenous malformations (AVMs).1, 2
Symptoms
Ischemic Stroke: Sudden dizziness, headache, nausea, vomiting, double vision, trembling, poor coordination, difficulty speaking or swallowing, and unconsciousness. 3, 4
Hemorrhagic Stroke: Sudden severe headache, loss of consciousness, nausea, vomiting, dizziness, balance issues, confusion, and unilateral weakness or numbness.3, 5, 6
Diagnosis
Physical examinations and diagnostic tools such as blood tests, carotid ultrasound, angiography, computed tomography (CT)/magnetic resonance imaging (MRI) scans, echocardiograms, and electrocardiograms (ECGs) are used to identify the type and location of a stroke. 1, 2, 8
Treatment
Hemorrhagic stroke
Rehabilitation and RecoveryRecovery often involves a multidisciplinary team comprising physicians, nurses, therapists, social workers, and psychologists. Interventions include:
Physical Therapy: To restore movement and strength 11, 12, 13
Occupational Therapy: To assist with activities of daily living 12, 13
Speech and Language Therapy: To improve communication and swallowing functions 12, 13
Cognitive and Emotional Support: Addressing memory deficits, depression, and anxiety 11, 7, 5, 3, 12, 13
Materials and Methods
Sources of data and materials
Patient case sheet.
Medication chart.
Laboratory data.
Progress reports.
Neurological assessment reports (standardized and self-designed) .
Suitable self-designed data collection form.
Method of collection of data
A comparative study was conducted on the patients according to the inclusion criteria after obtaining the consent form. All the inpatients were reviewed daily for their progress. The Patient demographic details such as name, age, gender, weight, educational status, lifestyle, economic status, social status, date of admission, complaints on admission, history of previous, comorbidities illness and medication, social history, nutritional data , progress data were collected.
The patient data were collected from medical records and the recovery data were collected from the progress charts and interviewing the patient with open ended questions. Collected data were recorded in a self-designed patient data collection form and were assessed by neurological assessment charts and with standard neurological assessment and stroke severity assessment scale (Glasgow coma scale, NIH stroke scale).
The data collected included the data obtained from the doctor’s notes, nurses notes, physiotherapists notes, nutritional assessment reports, laboratory investigational reports, drug interaction charts, adverse drug reaction charts and through open ended questions.
Statistical analysis
Data were collected and entered into Microsoft Excel 2019 software and interpreted with descriptive statistics which then provided for analysis of the report and expressed as counts and percentages in the form of tables, charts and graphs.
Statistical analysis of the collected data was done using IBM SPSS version 26 statistical software.
Results
Categorization of patients based on the type of stroke.
A total of 300 patients were enrolled, with 129 (43%) diagnosed with hemorrhagic stroke and 171 (57%) with ischemic stroke. Ischemic stroke cases were notably higher than hemorrhagic (Table 1).
Categorization of patients based on their age
Patients were divided into seven age categories, ranging from 35 to 105 in intervals of 10 years. Among the 300 patients, those aged 65-75 had the highest stroke incidence, while those aged 95-105 had the lowest (Table 2).
Comparative categorization of patients based on their age
Among the 300 patients, the 65-75 age group had the highest stroke incidence, with 35% in hemorrhagic and 49% in ischemic strokes. The 95-105 age group had the lowest, with only 0.58% in ischemic strokes (Table 3).
Table 3
Comparative categorization of patients based on the age.
Categorization of patients based on their gender
Of the 300 patients enrolled, 66% were male, showing a higher diagnostic rate for cerebrovascular accidents compared to females at 34% (Figure 1).
Comparative categorization of patients based on their gender
In comparing stroke types, hemorrhagic stroke showed a higher prevalence in males (75.2%) than females (24.8%). For ischemic stroke, males also had a higher rate (59.06%), while females accounted for 48.54% (Table 4).
Categorization of patients based on the length of hospital stay
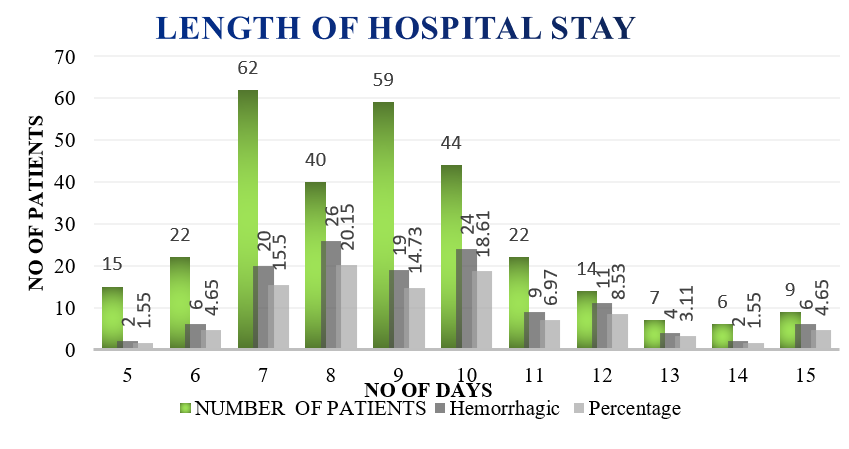
Among the 300 patients, 9 had the longest hospital stays (3%), while 15 had the shortest (5%). The most common length of stay was 7 days, with 62 patients (20.7%), followed by 9 days (59 patients, 19.7%) and 10 days (44 patients, 14.7%). Other notable stays included 8 days (40 patients, 13.3%), 6 and 11 days (22 patients each, 7.3%), and shorter stays of 5 days (15 patients, 5%). The fewest stays were 13-15 days, representing under 3% each (Table 5).
Comparative categorization of patients based on the length of hospital stay
In ischemic stroke (171 patients), 1.75% had the longest stay, 7.60% the shortest, and 7 days was the most frequent duration (24.57%). In hemorrhagic stroke (129 patients), 4.65% had the longest stay, 1.55% the shortest, and 8 days was most frequent (20.15%). Ischemic strokes had higher enrollment with shorter frequent stays (Figure 2).
Comparative categorization of patients with and without comorbidities
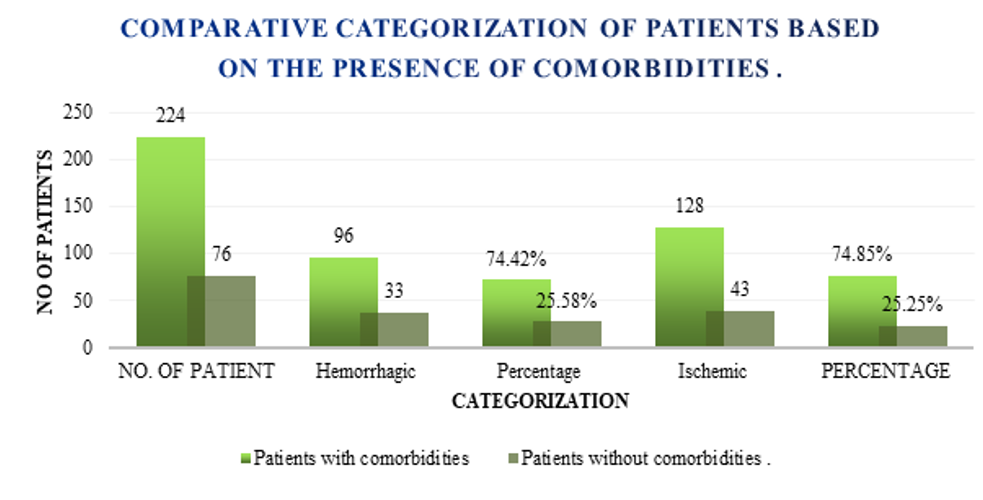
Out of the patients being enrolled in the study, on comparison between Haemorrhagic and Ischaemic strokes , out of the 129 Haemorrhagic patients , 33 (25.58 %) patients were seen without comorbidities and 96 (74.42%) patients were seen with comorbidities (Figure 3).
CNS examination of patients being enrolled
On admission, 286 patients were alert, 267 had anxiety, 131 had sensory neglect, 106 were lethargic, and 124 showed right-left confusion. Language, attention, and memory issues were seen in 130, 138, and 133 patients, respectively (Table 6).
Table 6
CNS examination of patients being enrolled
Possible risk factors observed in patients
Heart diseases (e.g., atrial fibrillation, 20.8%) were major risk factors, with high BP and diabetes common in hemorrhagic stroke. Lifestyle factors like obesity, and smoking were more significant in ischemic stroke, highlighting lifestyle’s role in stroke risk (Table 7).
Table 7
Possible risk factors observed in patients
Pre-assessment of stroke severity
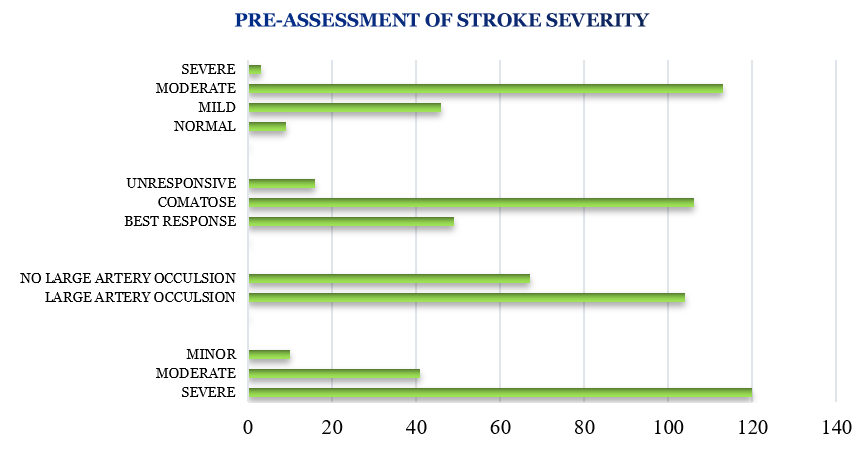
Among 171 ischemic stroke patients, admission showed severe impairment in most (120 NIH, 104 artery occlusion, 106 comatose). At discharge, 161 had minor strokes (NIH), 156 no occlusion, and 165 were normal (MMSE) (Figure 4).
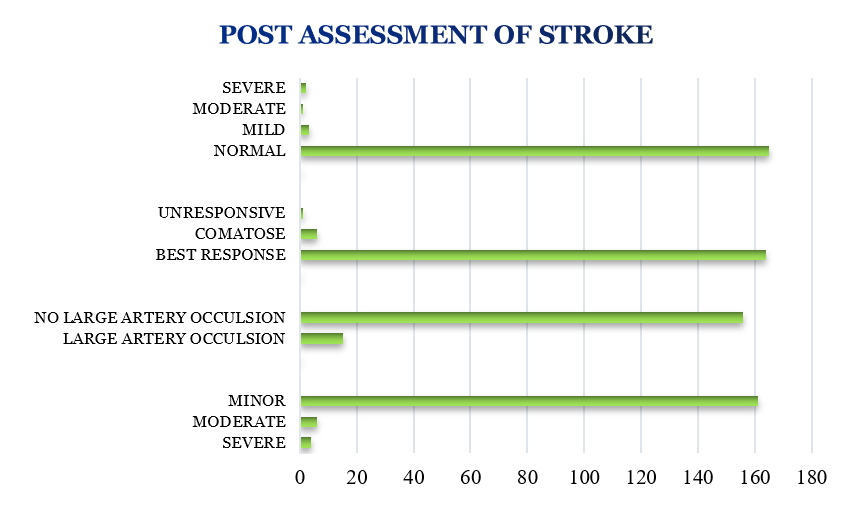
Post assessment of stroke severity
At discharge, 171 ischemic stroke patients showed significant improvement: 161 had minor strokes (NIH), 156 had no artery occlusion (Standard Scale), 164 showed the best response (Glasgow), and 165 were normal (MMSE) (Figure 5).
Comparison of pre and post stroke severity
Pre-Assessment of Stroke Severity: Upon admission of 171 ischemic stroke patients, 120 exhibited severe impairment on the NIHSS, 104 had artery occlusion, and 106 were comatose.
Post-Assessment of Stroke Severity: At discharge, 161 patients had minor strokes on the NIHSS, 156 showed no artery occlusion, and 165 were assessed as normal on the MMSE, indicating significant recovery.
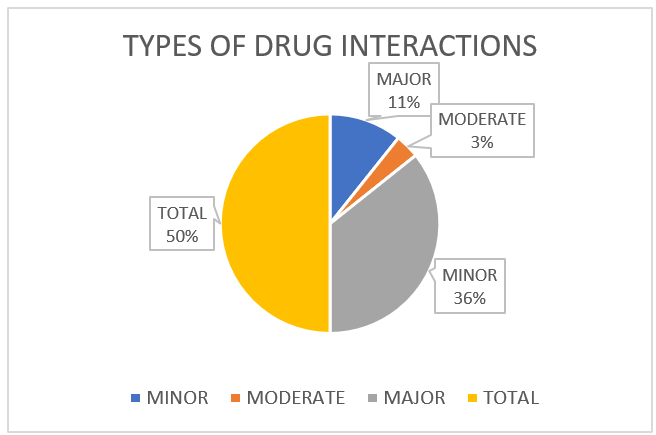
Drug interactions with percentage
On the study performed, total of 42 drug interactions were reported . 9 Major drug - drug interactions with 21.4% has been reported which is been followed by 30 minor drug - drug interactions with 71.4% and the least of it being the moderate drug - drug interactions with 7.1% reported in 3 patients (Figure 6).
Comparison of cost burden in patients with hemorrhagic and ischemic stroke
The cost burden comparison between hemorrhagic and ischemic stroke patients showed a higher burden in ischemic stroke, though no significant statistical difference was observed between the two types of stroke (Table 8).
Table 8
Comparison of cost burden in patients withhemorrhagic and ischemic stroke
Discussion
Stroke remains a leading cause of morbidity and mortality globally, highlighting the need for better understanding and management. This study provides valuable insights into ischemic and hemorrhagic stroke profiles, severity, and recovery. Our findings show that ischemic strokes (57%) are more prevalent than hemorrhagic strokes, in line with global trends, and age, especially 65-75 years, is a significant risk factor. The higher incidence of stroke in males (66%) supports previous studies on gender differences in stroke types.
Ischemic stroke patients generally had shorter hospital stays and significant improvement in severity, which emphasizes the effectiveness of early interventions. Comorbidities like hypertension, diabetes, and smoking were identified as key risk factors, underlining the importance of a multidisciplinary approach to care. Additionally, 42 drug interactions, including nine major ones, highlight the need for careful medication management.
Although ischemic stroke patients incurred slightly higher costs, the economic burden of stroke care is substantial. This study underscores the importance of early detection, personalized treatment, and comprehensive post-stroke care to improve outcomes and reduce healthcare costs.
Categorization of stroke type
Out of 300 patients, 43% had hemorrhagic strokes and 57% had ischemic strokes, with ischemic strokes being more common, in line with global trends.14, 2.
Age distributionThe majority (28%) of patients were in the 65-75 years age group, with a noticeable decrease in incidence among those aged 95-105 years, highlighting age as a significant risk factor.
Age and Stroke Type:The 65-75 years age group had the highest incidence of both stroke types, with ischemic strokes being more frequent than hemorrhagic strokes in all age groups.10, 9
Gender Categorization of Stroke Type:
Out of 300 patients, 43% had hemorrhagic strokes and 57% had ischemic strokes, with ischemic strokes being more common, in line with global trends.14, 2
Age distribution
The majority (28%) of patients were in the 65-75 years age group, with a noticeable decrease in incidence among those aged 95-105 years, highlighting age as a significant risk factor.
Age and stroke type
The 65-75 years age group had the highest incidence of both stroke types, with ischemic strokes being more frequent than hemorrhagic strokes in all age groups.10, 9
Gender distribution
66% of stroke patients were male, indicating a higher stroke incidence in males compared to females. 11
Gender and stroke type
Hemorrhagic strokes were more common in males (75.2%) compared to females (24.8%). Similarly, ischemic strokes also had a higher male prevalence (59.06%).7
Hospital Stay Duration
Most patients had hospital stays of 6-10 days, with a significant portion staying for 7 or 9 days.5
Stay duration by stroke type
Ischemic stroke patients tended to have shorter stays, with 24.57% staying for 7 days, while hemorrhagic stroke patients had slightly longer stays.3
CNS examination on admission
Most patients were alert on admission, with common neurological deficits including anxiety, sensory neglect, and lethargy.5
Risk factors
Hypertension, diabetes, and heart diseases like atrial fibrillation were key risk factors. Lifestyle factors such as anxiety and smoking were linked to ischemic strokes.10, 9
Pre-assessment severity
At admission, ischemic stroke patients showed significant neurological impairment, which improved by discharge, with most showing mild strokes.5
Post-assessment severity
Most ischemic stroke patients showed improvement, with many scoring as mild on the NIHSS and normal on the MMSE by discharge. 3
Drug interactions
42 drug interactions were identified, mostly minor, with nine major interactions, emphasizing the need for careful medication management. 11
Cost comparison
Ischemic stroke patients incurred slightly higher costs than hemorrhagic stroke patients, though the difference was not significant, highlighting the economic burden of stroke care. 7, 5
Distribution:66% of stroke patients were male, indicating a higher stroke incidence in males compared to females. 11
Conclusion
Our study compared hemorrhagic and ischemic strokes, revealing key findings: ischemic stroke had a higher prevalence (57%), and patients with ischemic strokes recovered faster than those with hemorrhagic strokes. Lifestyle factors such as smoking and alcohol use were identified as primary risk factors for ischemic strokes. The cost burden was similar for both stroke types, highlighting the significant economic impact of stroke care. Additionally, stroke rehabilitation and counseling played a crucial role in improving patient outcomes, emphasizing the importance of these interventions in enhancing recovery and informing effective stroke management strategies.